
Diagnostic Imaging ofAcute Bowel Pathology
Susan L Summerton, MD


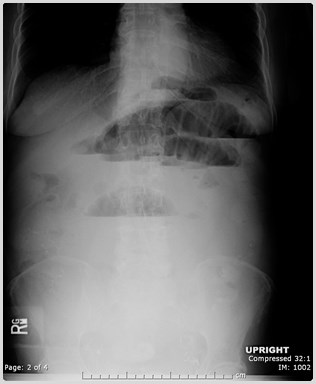
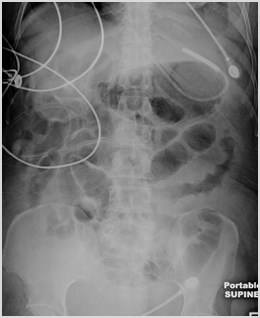
SUPINE
UPRIGHT

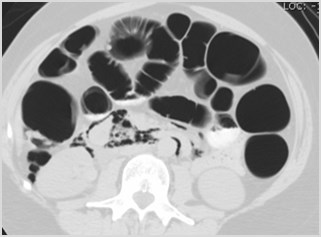
Dilated Loops ofSmall Bowel
Paucity of BowelGas in Colon
Multiple Air-Fluid Levels atDifferent Levels
Small Bowel Obstruction
SBO Imaging
•Plain films
•80-90% vs 30-70% accuracy
•Do not assess site or cause
•CT
•90% accuracy in suspected high grade SBO
•Identifies site and cause
•Most common cause is adhesions
–(with or without history of prior abdominal surgery)
•Identifies complications
•Small-bowel Follow-Through
•Problem solving tool
Contrast
•Oral – Controversial
-Delays diagnosis
-Aspiration risk
-Intravascular volumedepletion/ electrolyteimbalances
+Differentiates partial fromcomplete SBO
+Accelerates surgicaldecision in a completeSBO
•IV
•Always use unlesscontraindications
•Helpful in diagnosingbowel wall ischemia
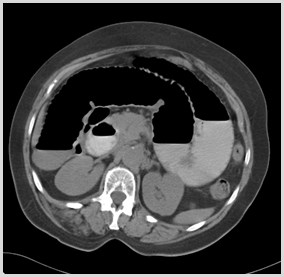
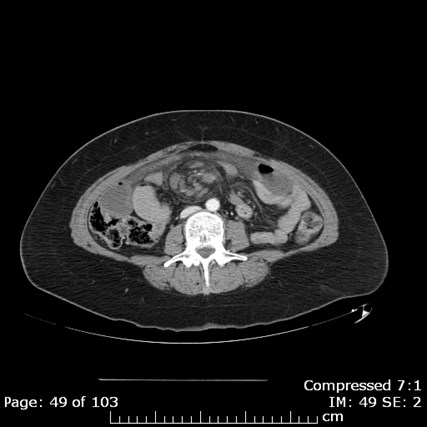
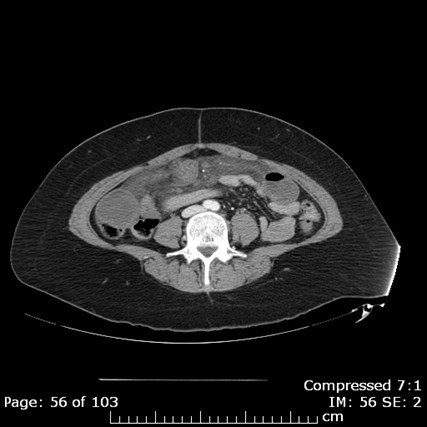
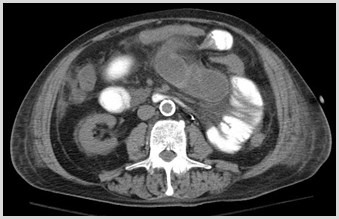
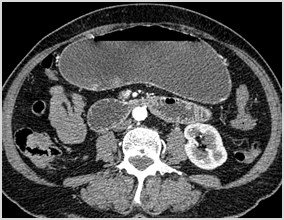
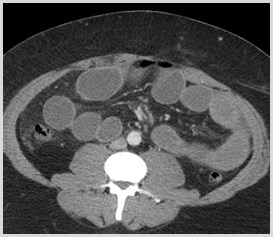
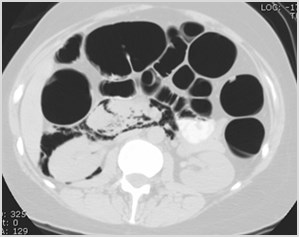
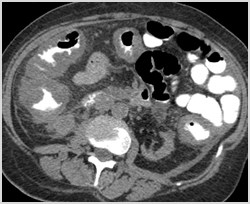
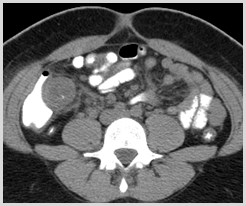
Small Bowel Obstruction:CT Findings
•Dilated loops of small bowel to atransition point
•Multiple air-fluid levels
•Progressive dilution of oral contrast
•Small bowel feces sign
•Whirl Sign
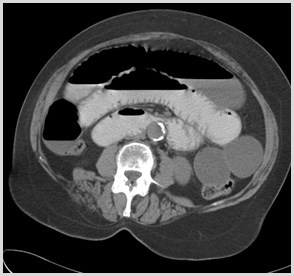
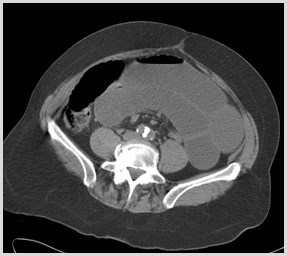
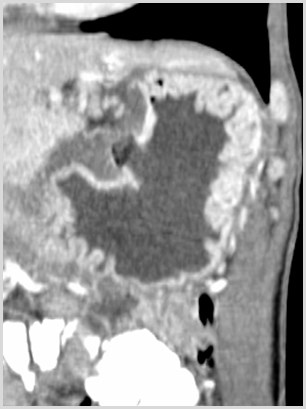
Small Bowel Feces Sign
•Present more frequently inpatients with moderate and highdegrees of SBO
•When present, can be used tolocate the transition point in SBO
Lazarus et al. Frequency and Relevance ofthe “Small-Bowel Feces” Sign on CT inPatients with Small Bowel Obstruction.AJR 2004; 183: 1361-1366

Whirl Sign
•T
w
i
s
t
o
f
b
o
w
e
l
w
r
a
p
p
i
n
g
a
r
o
u
n
d
a
s
i
n
g
l
e
c
o
n
s
t
r
i
c
t
i
v
e
f
o
c
u
s
o
f
m
e
s
e
n
t
e
r
y
•S
i
g
n
o
f
c
l
o
s
e
d
l
o
o
p
o
b
s
t
r
u
c
t
i
o
n
•I
n
d
i
c
a
t
e
s
p
o
s
s
i
b
l
e
c
o
m
p
r
o
m
i
s
e
/
c
o
m
p
r
e
s
s
i
o
n
o
f
v
a
s
c
u
l
a
t
u
r
e
•P
a
t
i
e
n
t
s
w
i
t
h
a
w
h
i
r
l
s
i
g
n
o
n
C
T
w
e
r
e
2
5
t
i
m
e
s
m
o
r
e
l
i
k
e
l
y
t
o
n
e
e
d
s
u
r
g
e
r
y
t
h
a
n
p
a
t
i
e
n
t
s
w
i
t
h
o
u
t
Duda et al. Utility of CT whirl sign inguiding management of small bowelobstruction. AJR 2008; 191: 743-747




















Whirl Sign
Closed Loop Obstruction
•10% of small bowel obstructions
•Mortality rate: 10-37%
•Complications
•Bowel strangulation
•Vascular compromise
•Ischemia/Infarction
Closed Loop Small BowelObstruction
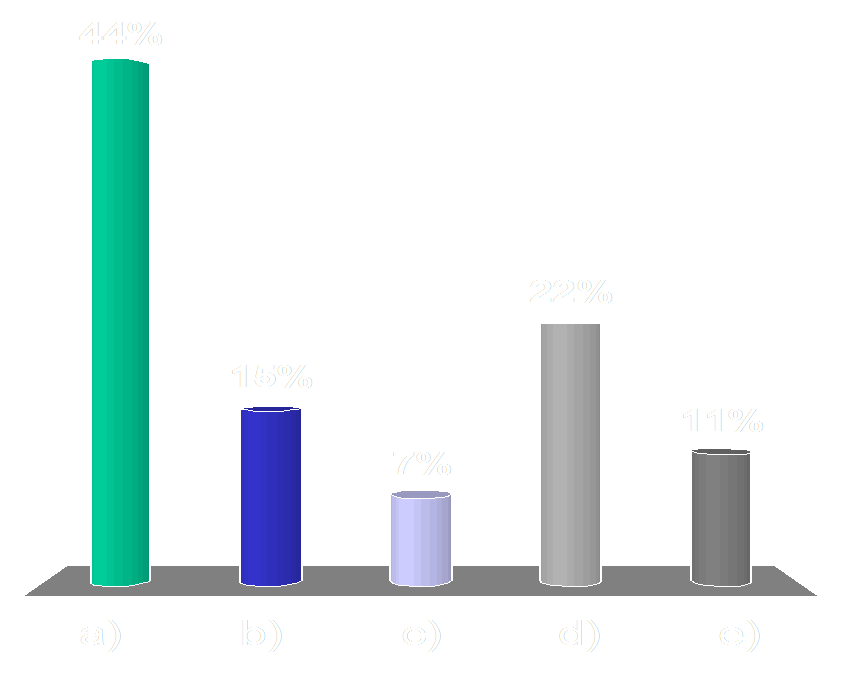
Which of the following causes of a smallbowel obstruction can be diagnosed only onCT and not on x-rays?
Audience Question
a)Adhesions
b)Hernia
c)Mass
d)Gallstone ileus
e)Abscess
Which of the following causes of a smallbowel obstruction can be diagnosed only onCT and not on x-rays?
Audience Question
a)A
d
h
e
s
i
o
n
s
b)H
e
r
n
i
a
c)M
a
s
s
d)G
a
l
l
s
t
o
n
e
i
l
e
u
s
e)A
b
s
c
e
s
s
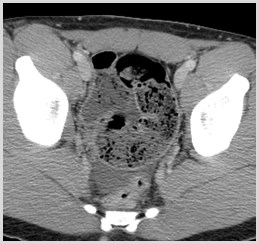
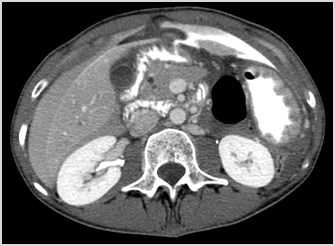
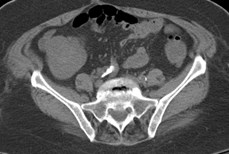
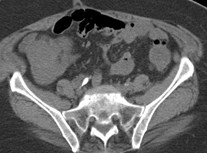
Causes of Small BowelObstruction
•Adhesions – only diagnosed on CT
•The adhesive band itself is not visible, butthe finding of abrupt change in caliberwithout other etiology (mass/hernia)implies adhesive band is present
•May be visible on x-rays
•Hernia
•Mass
•Intussusception
•Gallstone ileus
•Abscess/Hematoma



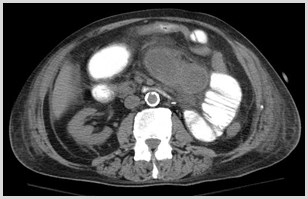
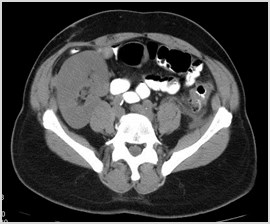
*
Dilated Proximal
Small Bowel
CollapsedColon
Collapsed Distal
Small Bowel

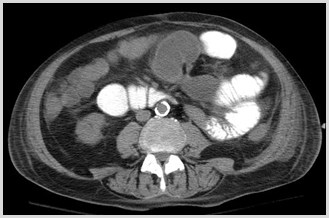
Proximal Dilated
Small Bowel
Distal Collapsed
Small Bowel
Transition Point
SBO - Adhesion
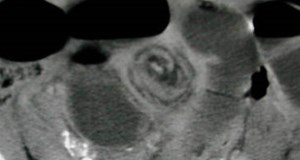
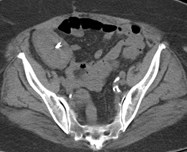
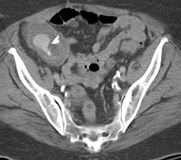
Intussusception
•Telescoping of one bowel loop into the lumenof an adjacent bowel loop
•Major cause of SBO in children
•Usually no lead point in children
•Adults often have tumor as lead point
•Symptoms
•Crampy abdominal pain
•Bloody stools
•Vomiting
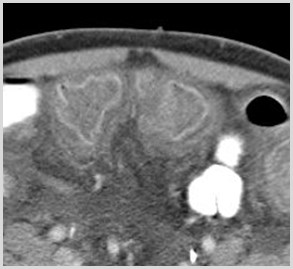
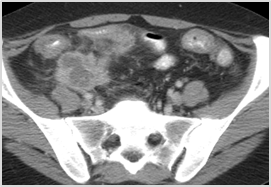
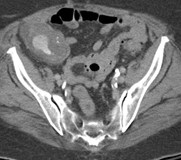
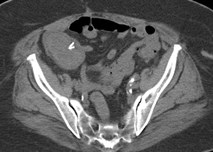
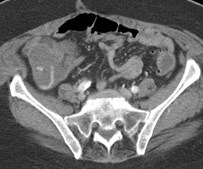
Intussusception: CT Findings
•Alternating bands of high & low density
•Results from intussuscepted mesenteric fatand mucosal-muscular interfaces
•+/- Bowel obstruction
Do we need to worry about every patientwith intussusception?
•33 adult patients with intussusception
•29/33 small bowel intussusception: only 6 hadneoplastic lead point
•4/33 colon intussusception: all had cancer
•Intussusception due to neoplasm:
•LONGER: 10.8 cm vs 4 cm long
•LARGER: 4 cm vs 3 cm
•More likely to obstruct: 50% vs 4.3%
Warshauer, DM et al. Adult Intussusception Detected at CT or MR Imaging:Clinical-Imaging Correlation. Radiology. 1999;212:853-860
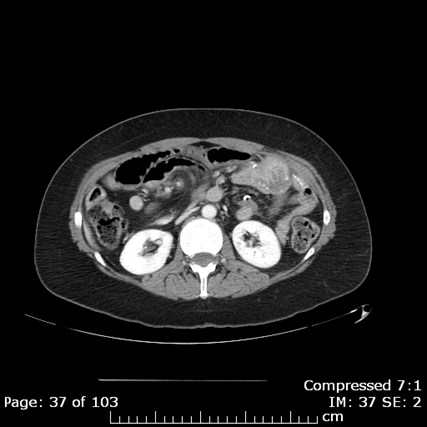
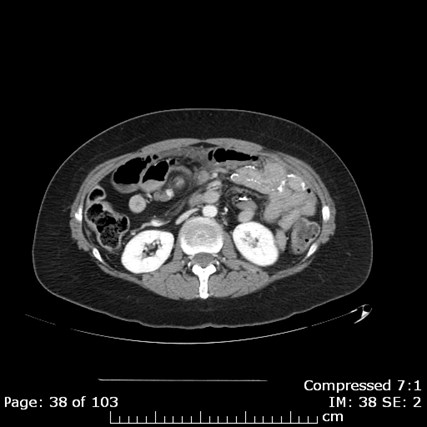
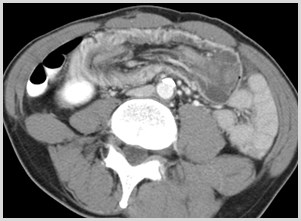
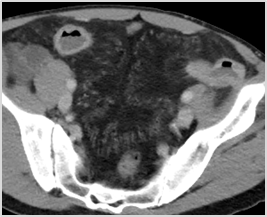
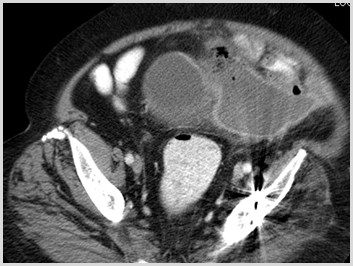
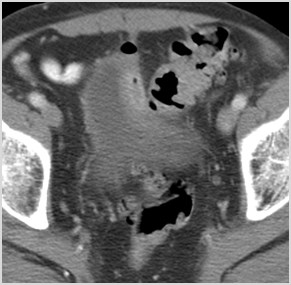
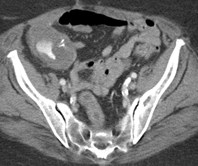
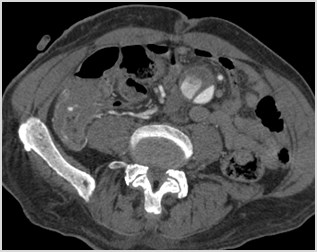
Jejunal mucinousadenocarcinoma



+
+
+


Dilated loops of smallbowel proximal
Small bowel feces sign
SBO
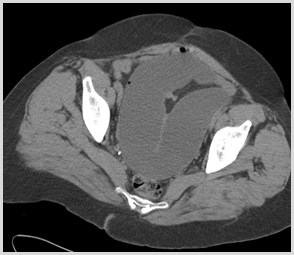
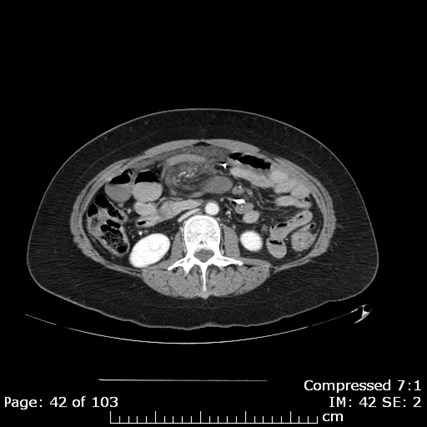
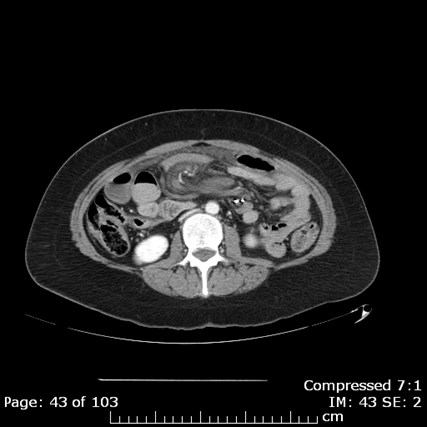
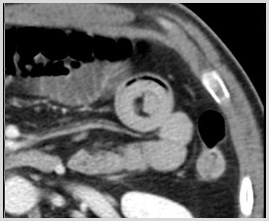
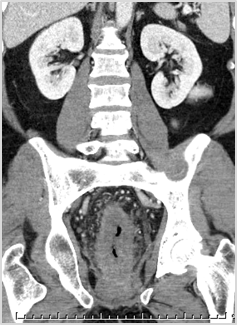
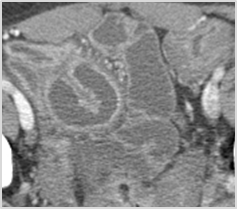
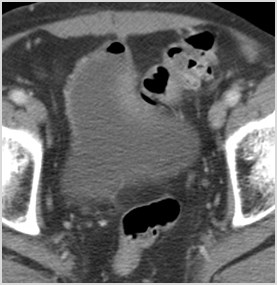
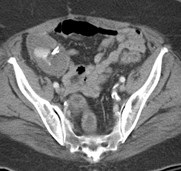
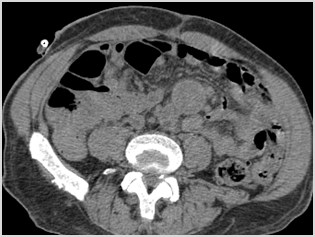
Paraumbilical
Hernia
Decompressed loops
of small bowel distal
SB protrudingthrough abd wall
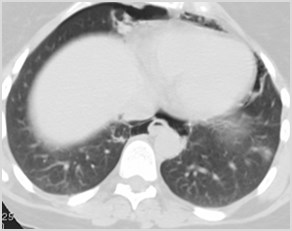
Bowel Perforation
•Small amounts of localized air
•Diverticulitis
•Appendicitis
•Cancer
•Large amounts of air
•Perforated gastric or duodenal ulcer
•Retroperitoneal air
•Perforated duodenum
Strong predictors of the site ofbowel perforation
•Focal defect in the bowel wall
•Concentration of extraluminal gas orcontrast adjacent to the bowel wall
•Segmental bowel wall thickening
Hainaux B et al. Accuracy of MDCT in Predicting Site ofGastrointestinal Tract Perforation. AJR 2006: 1179-1183

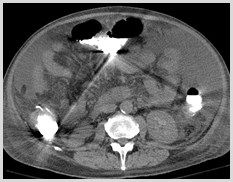
Perforated Duodenal Ulcer
Site of Perforation
Highest Density
Extraluminal Contrast
High Density
Perihepatic Fluid

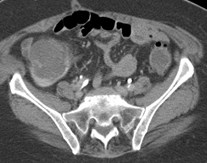
Retroperitoneal air due to duodenal perforation


Gastric Ulcer
Gastric Wall Thickening
Gastric Ulcer along the LesserCurvature

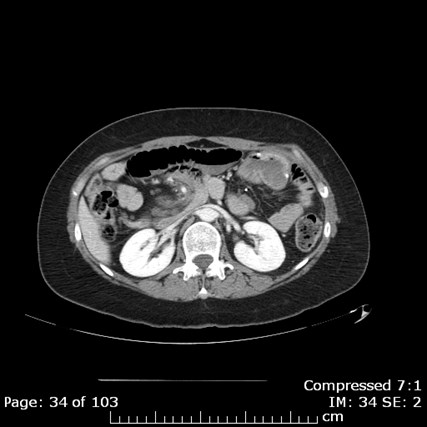
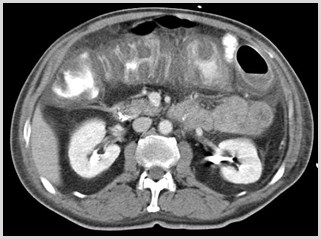
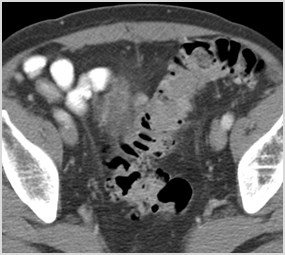
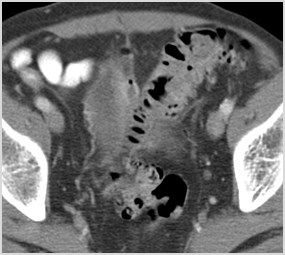
Colitis
•Infectious
•Pseudomembranous colitis
•Inflammatory
•Crohn’s
•Ulcerative colitis
•Ischemic
•Diverticulitis
Colitis
•CT of abdomen and pelvis with oral andintravenous contrast
•Findings are most often nonspecific
•Certain patterns/features on CT canhelp narrow the differential diagnosis
•Clinical and laboratory data
•Colonoscopy and biopsy

Colonic wall thickening
Radiation Proctitis
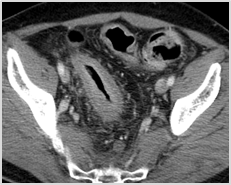


Target Sign
•Alternating bands of density in bowel wall
•Nonspecific/implies acute benign process
•Ischemia/ inflammatory/ infectious
Pseudomembranous Colitis
•Clostridium difficile
•Antibiotic use; Chemo
•Thumbprinting
•Accordion sign
•Ascites
•Often most severe degree ofwall thickening of colitides

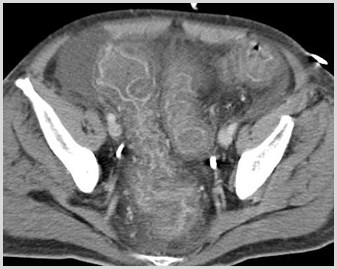
Crohn’s Disease
•Clinical manifestations
•Abdominal pain and diarrhea
•Weight loss and fever
•Bowel involvement
•Mouth to anus
•Small bowel: terminal ileum most common
•Small and large bowel – 50%
•Large bowel only – 20%
Crohn’s Disease
•Complications
•Bowel obstruction caused by strictures
•Fistulae
•enterocutaneous
•enterovesical
•enterovaginal
•Perforation with sinus tracts
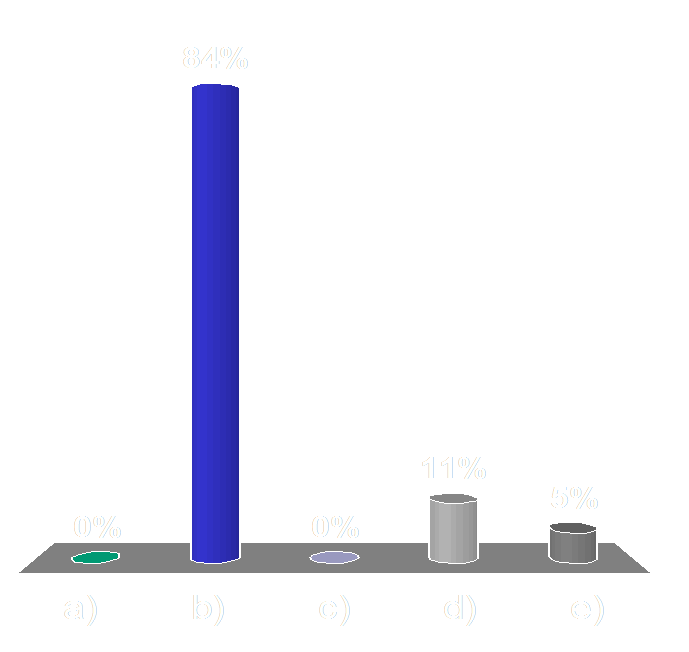
Which of the following studies in evaluating forCrohn’s disease exposes your patient to the leastamount of radiation?
Audience Question
a)CT Enterography
b)MR Enterography
c)Small bowel follow through
d)Barium enema
e)Plain radiographs of theabdomen
Which of the following studies in evaluating forCrohn’s disease exposes your patient to the leastamount of radiation?
Audience Question
a)C
T
E
n
t
e
r
o
g
r
a
p
h
y
b)M
R
E
n
t
e
r
o
g
r
a
p
h
y
c)S
m
a
l
l
b
o
w
e
l
f
o
l
l
o
w
t
h
r
o
u
g
h
d)B
a
r
i
u
m
e
n
e
m
a
e)P
l
a
i
n
r
a
d
i
o
g
r
a
p
h
s
o
f
t
h
e
a
b
d
o
m
e
n
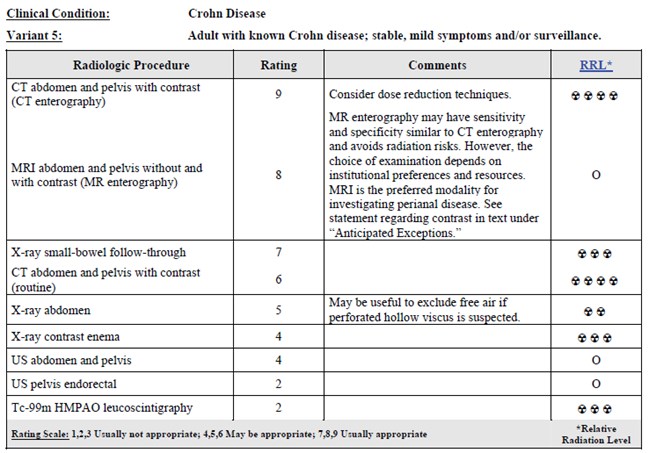
Role of Imaging
•Diagnosis
•Clinical, lab, histology
•Identify location andseverity
•Complications
•Following disease activity
•Monitoring therapy
Routine CT
SBFT
Enteroclysis
CT or MR
Enterography
Crohn’s Disease
Reprinted with permission of the American College of Radiology. No otherrepresentation of this material is authorized without expressed, writtenpermission from the American College of Radiology.
Crohn’s Disease: CT Findings
•Wall thickening with contrast enhancement
•Continuous or segmental (Skip lesions)
•Narrowed lumen (String sign)
•Increased fat around affected segments ofbowel (Creeping fat)
•Separation of bowel loops (Proud loop)
•Engorged mesenteric vessels (Comb sign)
•Complications: fistulae, abscesses
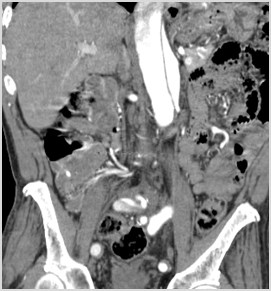
Crohn’s Disease


String sign
CT Findings


Creeping fat
Abscess
Engorged vasa recta
“comb sign”
Crohn’s Disease


Inflamed bowel
Thick walled
Submucosal enhancement
Normal
Ulcerative Colitis



Inflammatory Bowel Disease
Ulcerative Colitis
•Left sided or diffuse
•Rectum involved
•Continuous
•Backwash ileitis (dilated)
•No fistulae
•+ Strictures
•+ Abscess
Crohn’s
•Right sided or diffuse
•Rectum often not involved
•Discontinuous
•String sign (narrowed)
•+ Fistulae
•+ Strictures
•+ Abscess
Ischemic Colitis
•Older patients
•Causes
•Arterial occlusion
•Venous occlusion
•Non-occlusive (lower perfusion states)
•Distribution – “Watershed areas”
•distal transverse colon (Griffith’s point)
•distal descending colon (Sudeck’s point)
Ischemic Colitis
•CT angiogram of the abdomen andpelvis utilizing three phases
•Unenhanced
•Arterial
•Venous
•Most specific sign of bowel ischemia
•Non-enhancement of the bowel wall afteradministration of intravenous contrast
Pneumatosis Intestinalis
•High specificity for bowel infarction
•Intraluminal gas dissects throughdisrupted mucosa
•Translocation of bacteria - sepsis
•Gas can progress into
•mesenteric veins
•SMV
•portal veins
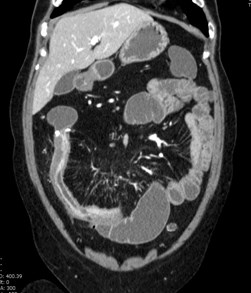
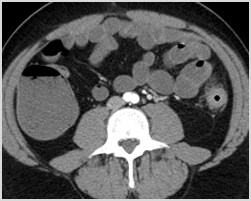
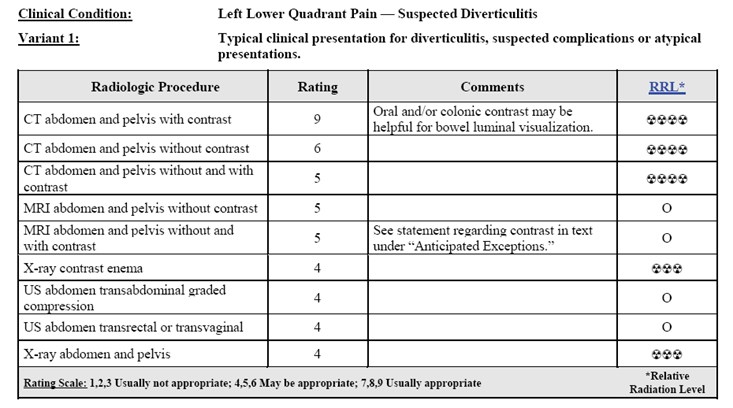
Colonic Diverticulitis
•Outpouchings of colonic mucosa/submucosa that become obstructed
•Most common: descending/sigmoid colon
•Clinical:
•LLQ pain
•elevated WBC
•fever
•+/- bleeding
Reprinted with permission of the American College of Radiology. No otherrepresentation of this material is authorized without expressed, writtenpermission from the American College of Radiology.
Diverticulitis: CT Findings
•Colonic wall thickening inpresence of diverticula
•Pericolonic fat stranding
•Phlegmon, extraluminal gas,abscess, and dependent freefluid

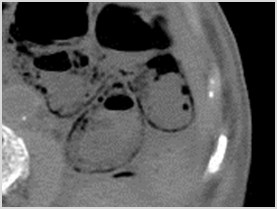
Complications of Diverticulitis
•Perforation
•Abscess
•Bowel obstruction
•Fistula formation
•Septic thrombophlebitis

Complications of Diverticulitis
Perforation and Abscess Formation
Locules of Free Air
Colovesicalfistulae
Acute LowerGastrointestinal Bleeding(LGIB)
Most Common Causes of LGIB
•Diverticular disease (20-55%)
•Angiodysplasia (3-40%)
•Neoplasms (8-26%)
•Colitis (6-22%)
•Benign anorectal lesions (9-10%)
Imaging Options
•Nuclear Medicine GI Bleed Study (0.1 mL/min)
•CT Angiography GI Bleed Study (0.3 mL/min)
•Conventional Angiography (0.5 mL/min)
•Colonoscopy
•Surgery
CT: Advantages
•A
v
a
i
l
a
b
l
e
a
n
d
R
a
p
i
d
l
y
A
c
q
u
i
r
e
d
•N
o
n
i
n
v
a
s
i
v
e
•P
r
o
v
i
d
e
s
b
e
t
t
e
r
l
o
c
a
l
i
z
a
t
i
o
n
•M
a
y
d
e
f
i
n
e
t
h
e
p
a
t
h
o
l
o
g
i
c
c
a
u
s
e
•E
v
a
l
u
a
t
i
o
n
o
f
v
a
s
c
u
l
a
t
u
r
e
•R
e
d
u
c
e
a
n
g
i
o
t
i
m
e
/
#
o
f
r
u
n
s
•R
e
d
u
c
e
a
n
g
i
o
c
o
n
t
r
a
s
t
d
o
s
e
•R
e
d
u
c
e
a
n
g
i
o
r
a
d
i
a
t
i
o
n
CT
•Sensitivity: 79-91%
•Specificity: 50-99%
•Diagnostic accuracy: 74-98%
CT: Limitations
•Renal failure
•Prior contrast reaction
•Residual oral contrast in bowel



Residual Contrast
Nuclear Medicine: Advantages
•Image over time
•Can use if IV contrast allergy
•Can use with elevated GFR
•Active arterial or venous bleeding ratesas low as 0.1 mL/min
•93% sensitive
•95% specific
Nuclear Medicine: Limitations
•Limited resolution
•Limited availability
•Length of time required to perform study
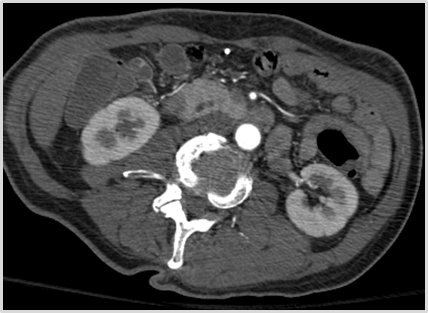
CT of Acute LGIB
•No oral contrast
•Scout – radiologist checks beforeproceeding with rest of study
•Low dose non contrast Abd & Pelvis
•Arterial Phase Abd & Pelvis
• 100-150 cc Optiray 320 at 4 cc/sec
•Venous: Abd & Pelvis -70 sec delay
Diagnosis of Bleeding
•High attenuation material detected within bowellumen at CTA, not present at unenhanced CTperformed immediately prior (Laing et al)
•Linear, jetlike, pooled or swirled or ellipsoid focalcollection of arterial density contrast materialwithin bowel lumen (Tew et al)
1.Tew K, Davies RP, Jadun CK, Kew, J. MDCT of Acute LowerGastrointestinal Bleeding. AJR 2004; 182: 427-430.
2.Laing CF, Tobia T, Rosenblum DI et al. Acute Gastrointestinal Bleeding:Emerging Role of Multidetector CT Angiography and Review of CurrentImaging Techniques. Radiographics 2007; 27: 1055-1070.





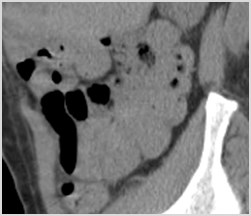

Coronal
SagittalCecum





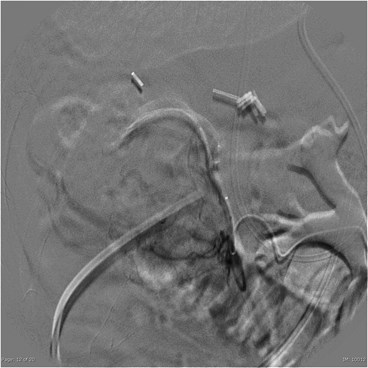
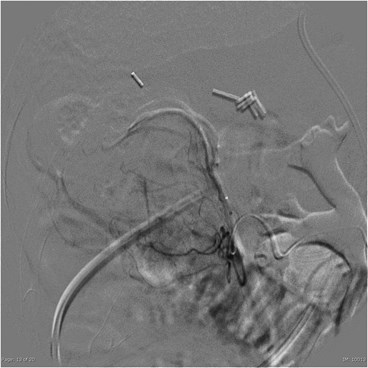
Catheter Angiography









References
1.Small Bowel Obstruction: What to Look For: AC Silva, M Pimenta, LSGuimaraes, RadioGraphics 2009; 29: 423-39.
2.Utility of CT whirl sign in guiding management of small bowelobstruction. Duda et al. AJR 2008; 191: 743-747
3.Acute Gastrointestinal Bleeding: Emerging Role of Multidetector CTAngiography and Review of Current Imaging Techniques. Laing CF,Tobia T, Rosenblum DI et al. Radiographics 2007; 27: 1055-1070.
4.Detection of active gastrointestinal hemorrhage with CT angiography: a4(1/2)-year retrospective review. Kennedy DW, Laing CJ, Tseng LH,Roseblum DI, Tamarkin SW. J Vasc Interv Radiol 2010; 21(6): 848-855.
5.CT Diagnosis of Acute Mesenteric Ischemia from Various Causes. AFurukawa, S Kanasaki, et al. American Journal of Roentgenology.2009;192: 408-416.